
 Article contributed by Ms Yong Lai Mee
Article contributed by Ms Yong Lai Mee
The prevalence of Type 2 Diabetes Mellitus (T2DM) among women in childbearing age is increasing. Pre-existing T2DM in pregnancy increased the risk of maternal and neonatal complications such as macrosomia big baby), miscarriage, stillbirth, eclampsia (high blood pressure and its complications), and preterm labour. The American College of Obstetricians and Gynaecologists and the American Diabetes Association emphasized the importance of achieving optimum diabetes control for promoting the well-being of maternal and reduced prenatal fetus and baby adverse outcomes. Below are some tips to achieve optimum pre pregnancy diabetes care.
Blood Glucose Control
- Keep pre pregnancy HbA1C < 6.5% to avoid complications during pregnancy.
- Fetal mortality rate increased 4 folds in those with HbA1C >6.6%.
- Poorly controlled pre pregnancy diabetes increases congenital heart diseases by 3 folds, neural tube defects increase by 4 folds and spontaneous miscarriages in 30-60% of all pregnancies.
- Plan 4-6 months before pregnancy to ensure diabetes control is within target range.
Blood Glucose Monitoring

- Aim for Fasting Blood Glucose < 6mmol/mol and 2 hours after meal <8mmol/L.
- Check blood glucose daily, frequency 4 to 7 times daily include Fasting Blood Glucose and 2 Hour Post Meal and Bedtime.
- Learn how to self check and monitor blood glucose.
- Active involvement of care and self-care yield better diabetes control.
Healthy Dietary Plan
Consume an appropriate amount of carbohydrate to suit lifestyle, maintain blood glucose control and ideal body weight. The total amount of carbohydrate (CHO) intake can be monitored using grams, exchange list, household, or hand measures. Below is a table of practice guide recommended by American Diabetes Association. (Every exchange consists of 15g Carbohydrate). You can get more information from these links HERE and HERE

- Plan for protein 15-20% total energy of the day such as lean meat, fish, chicken without skin or soy protein.
- Limit total fat (25%-35% energy intake), saturated fats (<7% energy intake) and minimize trans-fat (<1% energy intake). Limit intake of saturated fat, such as red meat and processed meat consumption.
- Have high fiber diet (20-30 gm fibre/day) by choosing plant-based foods such as vegetables, fruits, legumes and whole grain cereals.
- Avoid consumption of sugar-sweetened beverage, replace it with plain water.
- Follow the Malaysian Healthy Plate Model may help increase consumption of vegetables and fruits limit total fat (25%-35% energy intake), please see the diagram below.
- Consult a dietician to develop an individualised dietary plan.


Physical Activities
- Increased physical activity to improve diabetes control, weight maintenance, and reduce the risk of cardio-vascular disease.
- Choose activities that likely to maintain e.g brisk walking.
- Exercise at least 3 times/week, preferably most days of the week and with no more than 48-72 hours without physical activity.
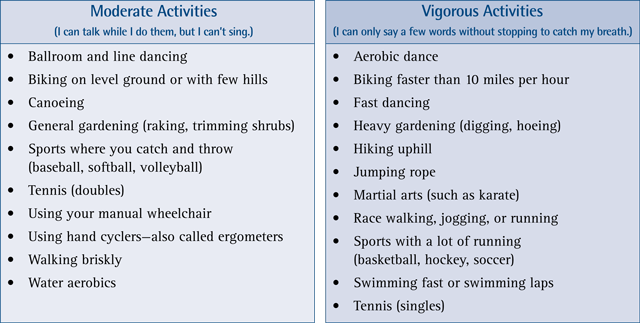
- The duration of exercise should be at least 150 minutes/week of moderate-intensity or at least 75 minutes/week of vigorous aerobic physical activity and at least 2 sessions per week of resistance exercise.
Obesity
- Obesity increased the risk of T2DM development in children bearing age women.
- The recommended ideal BMI is 18 to 23kg/m2 and waist circumference <80cm for women.
- A Weight loss of >7% -10% of body weight within 6 months has been proven to be effective in reducing HbA1C. This can be achieved by :

- Reduce calorie intake of 500-1000kcal/day from baseline. Eg aim for an intake of 1200 to 1500 kcal/day.
- Increase exercise to ≥60 minutes per day/approximately 450 minutes per week.
- A combination of reduced-calorie diet, physical activity and behavior modification can provide greater initial weight loss.
- Use Meal Replacement Plans as part of the structured meal plan. The meal replacement product is usually a milk drink formulated with controlled quantities of calories and nutrients intended to substitute solid food meal. Check with the doctor for the meal replacement product.
Medication
1.Diabetic Medications
- Oral diabetic medications are commonly prescribed for women with T2DM before pregnancy.
- Metformin has minimal effect on the fetus but may increase the risk of prematurity and associated with larger offspring.
- Sulphonylurea is associated with increased risk for baby developing low blood sugar level after delivery.
- There was inadequate data to evaluate the safe use of Sodium-glucose Linked Transporter 2 (SGLT2) Inhibitors, Dipeptidyl Peptidase-4 (DPP4) Inhibitors and Glucagon-like Peptide-1 (GLP1 – injection) receptor agonists.
- Due to the teratogenic (causing abnormalities to baby) effect of many oral diabetic medications, doctors preferred to switch diabetes treatment to insulin therapy prior to pregnancy.

2. Vitamins
Folic acid is important for pregnancy to prevent miscarriage and neural tube defects such as spinal bifida. Therefore, women should start taking it at least 3 months prior to pregnancy.
3.High Blood Pressure and Cholesterol Medications
- High blood pressure medication such as ACE inhibitors, Angiotensin II receptor blockers (ARBs) and cholesterol medications like statins will be discontinued due to the teratogenicity effect.
- Therefore, it is important to discuss with your doctor prior to embarking on pregnancy so that the high blood pressure medication can be switch to those that are proven safe in pregnancy.
- It is important to monitor home blood pressure daily and document the readings.
4.Insulin therapy
- Insulin is safe in pregnancy and not associated with fetal abnormalities.
- Before pregnancy, an intensive insulin therapy is likely to be initiated in the form of a multiple-dose injection treatment to achieve good blood glucose target.
- It is important to attend diabetes education session to learn the proper technique of insulin injection and understand how insulin work.

Eye Check
The risk of retinopathy progress may double during pregnancy.
Consult an Ophthalmologist for eye assessment. If eye problem is present, appropriate treatment will be provided.
Smoking and Alcohol

- Women who smoke during pregnancy increased the risk of fetal death by 91%.
- Alcohol consumption during the 1st-trimester increases the risk of abortion by 4 folds and precipitate preterm labor.
- Quit smoking and alcohol prior to conception.
Vaccination
 Vaccination is important to prevent communicable diseases. Vaccination is done according to the national clinical guideline recommendation. Click HERE for more info.
Vaccination is important to prevent communicable diseases. Vaccination is done according to the national clinical guideline recommendation. Click HERE for more info.
Preconception Counseling
- Pre pregnancy diabetes counseling empowered individual with the knowledge of diabetes self-care. This session should be done at least 4-6 months before pregnancy allowing time for a medication review and lifestyle modification to achieve optimal glycaemic control.
- See an Endocrinologist, a Diabetes Educator, and Dietician for the pre-pregnancy counseling.
Conclusion

Optimum pre-pregnancy Care in T2DM reduces the risk of complications during pregnancy. Pre-pregnancy care should be planned with a multidiscipline healthcare team at least 4-6 months prior to conception.
Article contributed by:
Ms Yong Lai Mee
President, Malaysian Diabetes Educators Society
Manager Diabetes Care Services/ Diabetes Educator
Subang Jaya Medical Centre
References and further reading:
- American Diabetes Association (ADA). (2020) Management of Diabetes in Pregnancy: Standards of Medical Care in Diabetes 2020. Diabetes Care. 43(Suppl. 1): S183-S192.
- American Diabetes Association (ADA). (2019) Classification and Diagnosis of Diabetes: Standards of Medical Care in Diabetes 2019. Diabetes Care. 42(Suppl.1): S65-S172.
- Bashir, M., Dabbous, Z., Baagar, K. et. al. (2019) European Journal of Obstetrics & Gynaecology and Reproductive. 233:53-57.
- Bhuvaneswar, C.G., Chang, G., Epstein, L. A. and Stern, T. A. (2007) Alcohol use during pregnancy: Prevalence and Impact. Primary Care Companion Journal of Clinical Psychiatry. 9,6:457-470.
- Blum, A. K. (2016) Insulin use in pregnancy: An update. Spectrum. 29,2:92-97.
- Etomi, O. & Banerjee, A. (2018) The management of pre-existing (type 1 and type 2) diabetes mellitus in pregnancy. Medicine and Other Specialties. 46,12:731-737
- Klein, J., Boyle, J.A., Kirkham, R., et al. (2017) Preconception care for women with type 2 diabetes mellitus: A mixed-methods study of provider knowledge and practice. Diabetes Research and Clinical Practice. 129:105-115.
- Ministry of Health (2020). Clinical Practice Guidelines: Management of type 2 Diabetes Mellitus.
Ministry of Health (MOH). (2017) Clinical Practice Guidelines: Management of Diabetes in Pregnancy. - Miodovnik, M., Lavin, J.P., Knowles, H.C., et al. (1984) Spontaneous abortions among insulin-independent diabetic women. American Journal of Obstetrics and Gynaecologists. 150:372-375.
- National Institute for Health and Care Excellence (NICE). (2015) Diabetes in Pregnancy: management from preconception to the postnatal period. NICE Guideline NG3, recommendation 1.1.11.
- Nagandla, K., Somsubhra, D. and Sachchithananthan, K. (2013) Oral hypolgyceamia agents in pregnancy: Update. Journal of Obstetrician Gynaecology Indian. March-April, 63,2:82-87.
National Institute for Health and Care Excellence (NICE) (2015) Diabetes in pregnancy: management from preconception to the postnatal period. - Shearer, D. and White, A. (2018) Preconception Management of Diabetes. BC Medical Journal. 6,5: 253-257.
- Roman, M. (2011) Preconception care for women with preexisting type 2 diabetes. Clinical Diabetes. 29,1:10-16.
- Shearer, D., White, A., Thompson, D. and Pawlowska, M. (2018) Preconception Management in Diabetes. British Columbia Medical Journal. 60,5:253-257.
- Temple, R.C., Aldridge, A.J. and Murphy, H.R. (2006) Pre-pregnancy care and pregnancy outcomes in women with Type 1 Diabetes. Diabetes Care. 29,8:1744-1749.
- Tennant, P.W.G., Glinianaia, S.V., Bilous, R.W. et. al. (2013) Pre-existing diabetes, maternal Glycated haemoglobin, and risks of fetal and infant death: a population-based study. Diabetologia. 57: 285-294. https://doi.org/10.1007/s00125-013-3108-5.
- Unger, J. (2007) Diabetes Management in Primary Care. Lippincott William & Wilkins. New York.
To print a pdf copy, click HERE.

[mailerlite_form form_id=3]